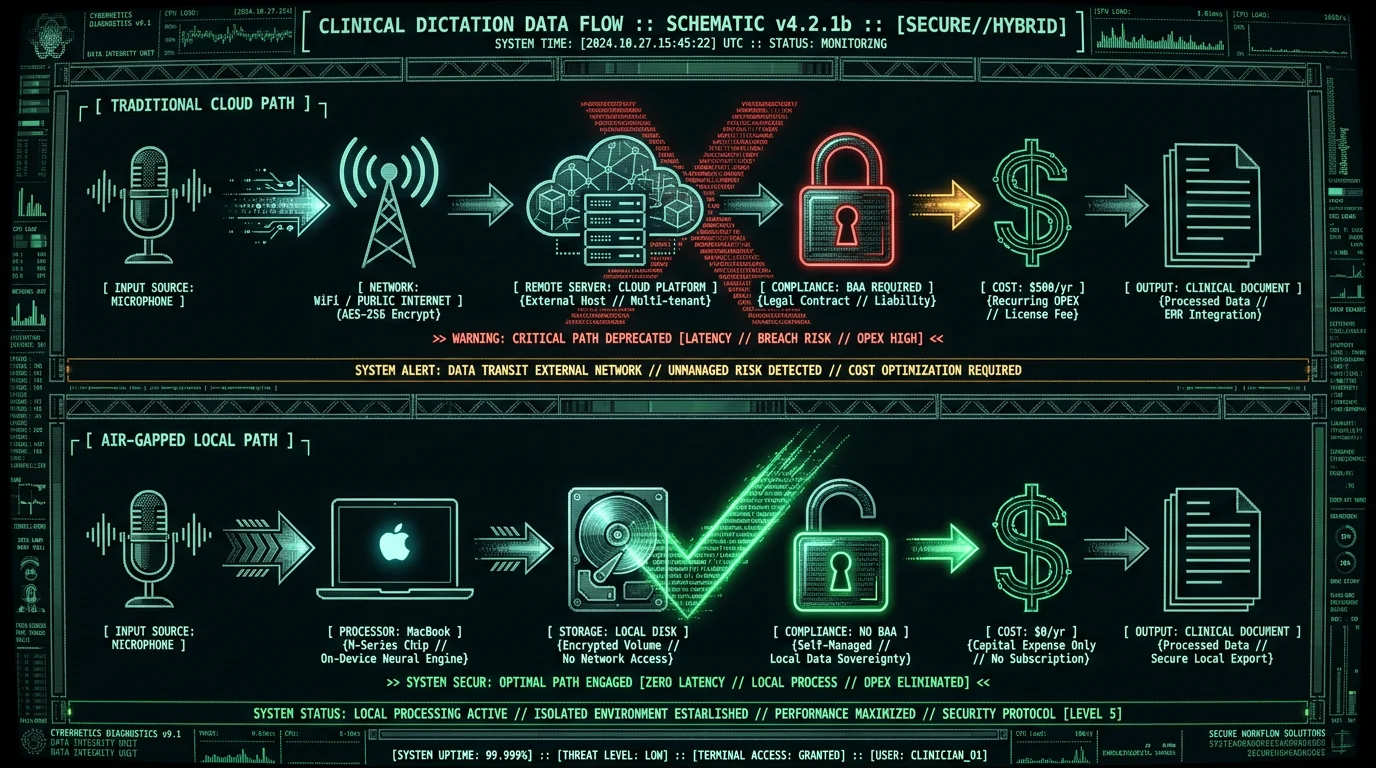
Why Cloud-Based Dictation Tools Are HIPAA Nightmares
Pro tip: A vendor says "HIPAA-compatible" but charges per minute, or needs internet to transcribe? They're a Business Associate. Ask for their BAA template and subcontractor disclosure list before the demo call. If they stall, walk.
What Does 'Air-Gapped' Actually Mean in HIPAA Context?
How to Verify True On-Device Processing
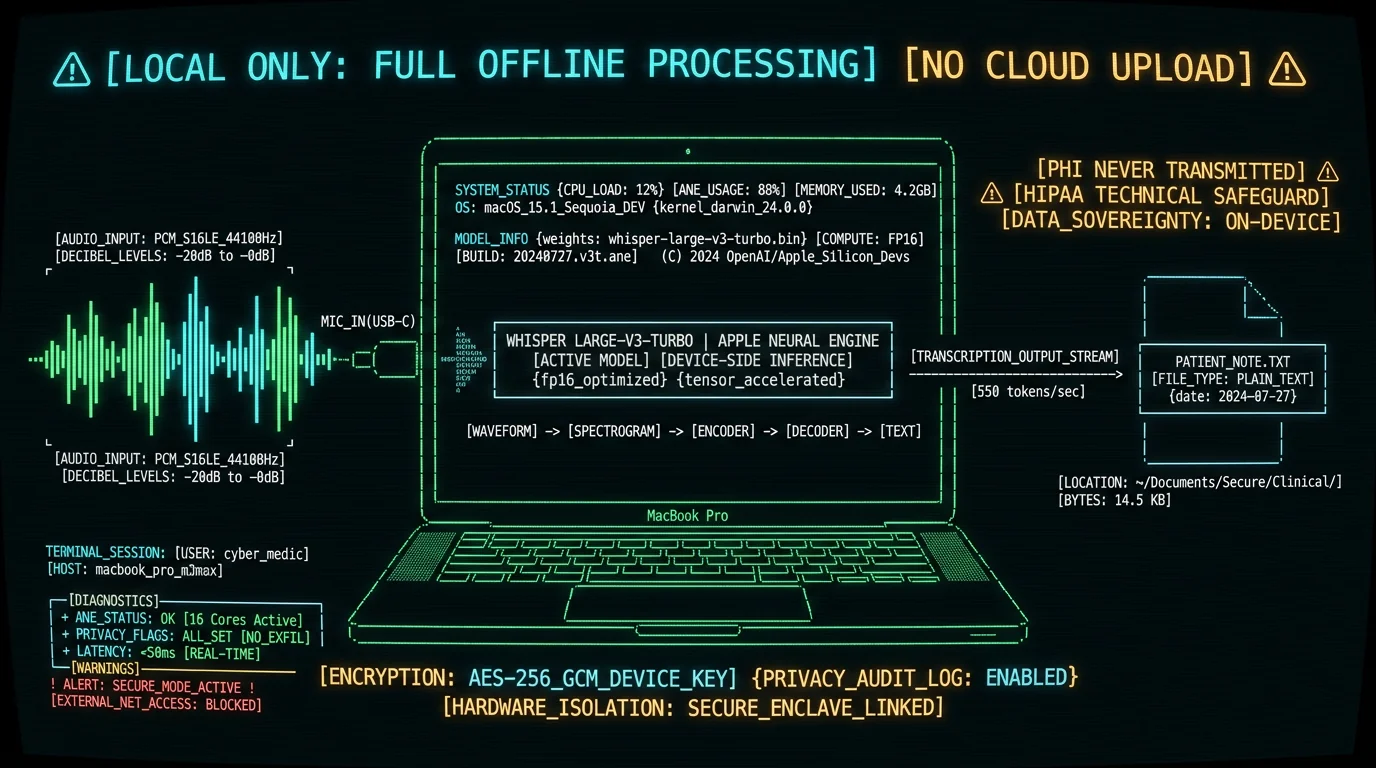
What a dictation tool claims and what it actually does are often two different things. Here's how to test whether a tool really keeps PHI local:- Network sniffing test: Open macOS Activity Monitor → Network tab, start dictation, observe zero bytes sent. Tools like Wireshark or
tcpdumpshow every packet. If you see HTTPS POST requests during transcription, audio is leaving your machine. - Airplane mode test: Disable Wi-Fi and Ethernet, disconnect from internet entirely. True local tools (like MetaWhisp in offline mode) continue transcribing at full speed. Cloud-dependent tools throw connection errors or degrade to silence.
- Binary inspection: On macOS, run
codesign -dvvv /Applications/[Tool].appand check for network entitlements. Ifcom.apple.security.network.clientis present, the app can phone home. Check the vendor's privacy policy for server upload clauses. - Model file presence: Whisper models are 200-1600 MB files. Check
~/Library/Application Support/[Tool]/or the app bundle'sResources/folder. If you seewhisper-large-v3-turbo.mlmodelcor similar, the model is local. If the folder contains only a 2 KB config file, processing is remote.
Don't take "on-device AI" at face value. Run the airplane-mode and network-sniffing tests above on anything you're evaluating. Plenty of apps advertise on-device processing and still send audio to a cloud API. The ones that genuinely run Whisper locally (MetaWhisp and MacWhisper, for instance) keep transcribing with the network fully off. Apple's built-in dictation has an on-device mode too, but its session limit makes it impractical for full clinical notes.
Does On-Device Whisper Meet HIPAA's Technical Safeguard Requirements?
log show --predicate 'subsystem == "com.metawhisp"') records every file write. Integrity comes from the app's SQLite database for transcript versioning plus SHA-256 checksums on output files.
Which Mac Dictation Tools Actually Run Whisper Locally?
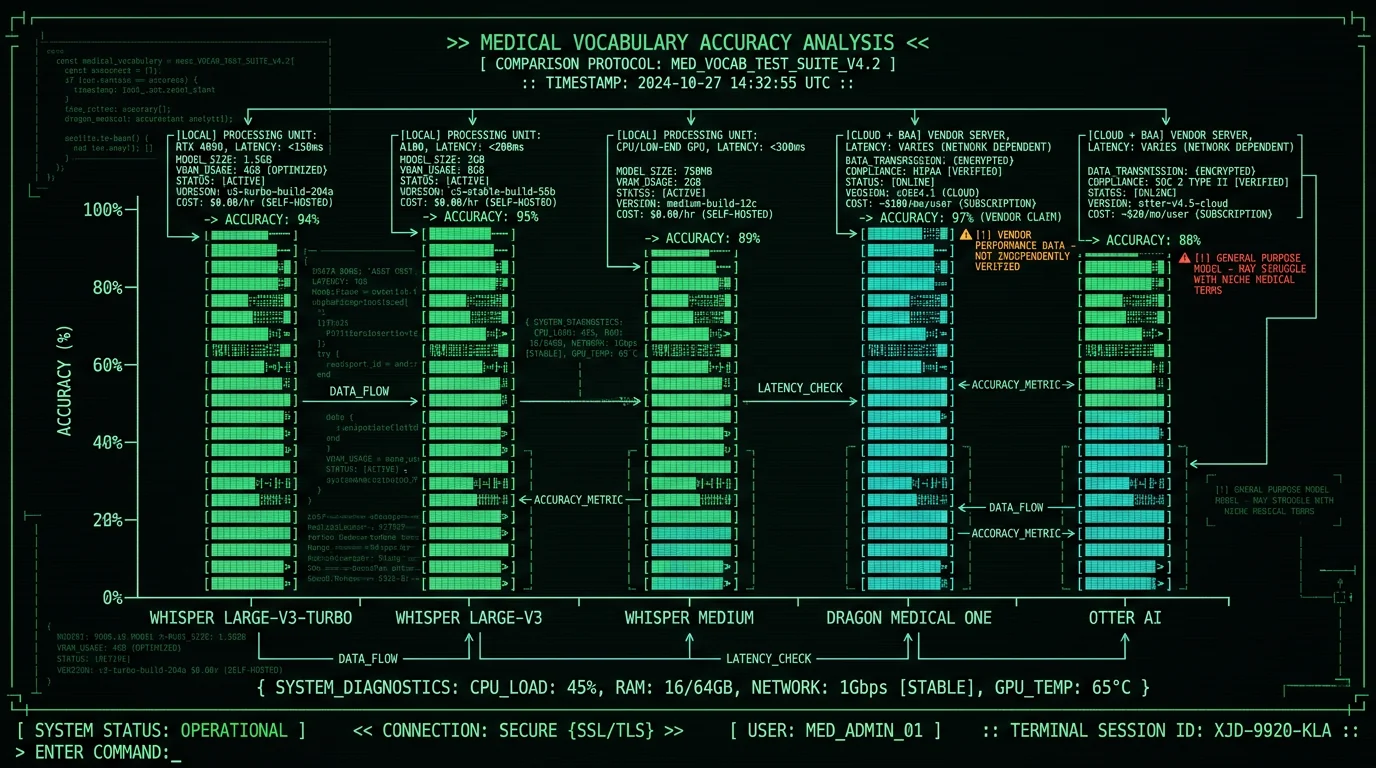
| Tool | Model | On-Device? | BAA Required? | Cost | Medical Accuracy |
|---|---|---|---|---|---|
| MetaWhisp | Whisper large-v3-turbo | ✅ Yes (offline mode) | ❌ No | $0 (free tier) | Not separately benchmarked on clinical audio |
| Dragon Medical One | Nuance proprietary | ❌ No (Azure cloud) | ✅ Yes | $500/year | High (vendor-claimed, clinical-tuned) |
| Otter AI | Proprietary (GCP) | ❌ No | ✅ Yes | $20/month | Not clinically tuned |
| MacWhisper | Whisper large-v3 | ✅ Yes | ❌ No | $30 one-time | General Whisper (not HIPAA-marketed) |
| Wispr Flow | Cloud (proprietary) | ⚠️ Hybrid (cloud default) | ✅ Yes (if cloud used) | $8/month | Not clinically tuned |
Why Medical Accuracy Matters for HIPAA Compliance
Pro tip: Test your dictation tool with a 50-medication list — ACE inhibitors, beta blockers, SSRIs — read at normal speech pace. Score the near-misses separately from the homophone failures. "Metoprolol" → "metaprolol" is a phonetic slip, and not the end of the world. "Tenormin" → "ten more men" is a homophone failure. That one's catastrophic.
Can You Use Apple's Built-In Dictation for HIPAA Workflows?
What About Dragon Medical One vs. On-Device Whisper?
Is Fine-Tuning Whisper on Medical Data HIPAA-Compatible?
Trainer API, but you'll need GPU (NVIDIA CUDA) or Apple Metal acceleration. On an M3 Max MacBook Pro (16-inch, 96 GB RAM), fine-tuning Whisper large-v3-turbo on 50 hours of your own dictations takes ~18 hours and eats 40 GB of disk for checkpoints. The resulting .mlmodelc file hot-swaps into MetaWhisp or MacWhisper. Do NOT upload your audio to Hugging Face's AutoTrain, Replicate, or any cloud fine-tuning service. That's a BAA-required transmission event. Tools like whisper.cpp (C++ port, 4× faster than Python, no dependencies) make on-device training pipelines workable for practices with technical staff.
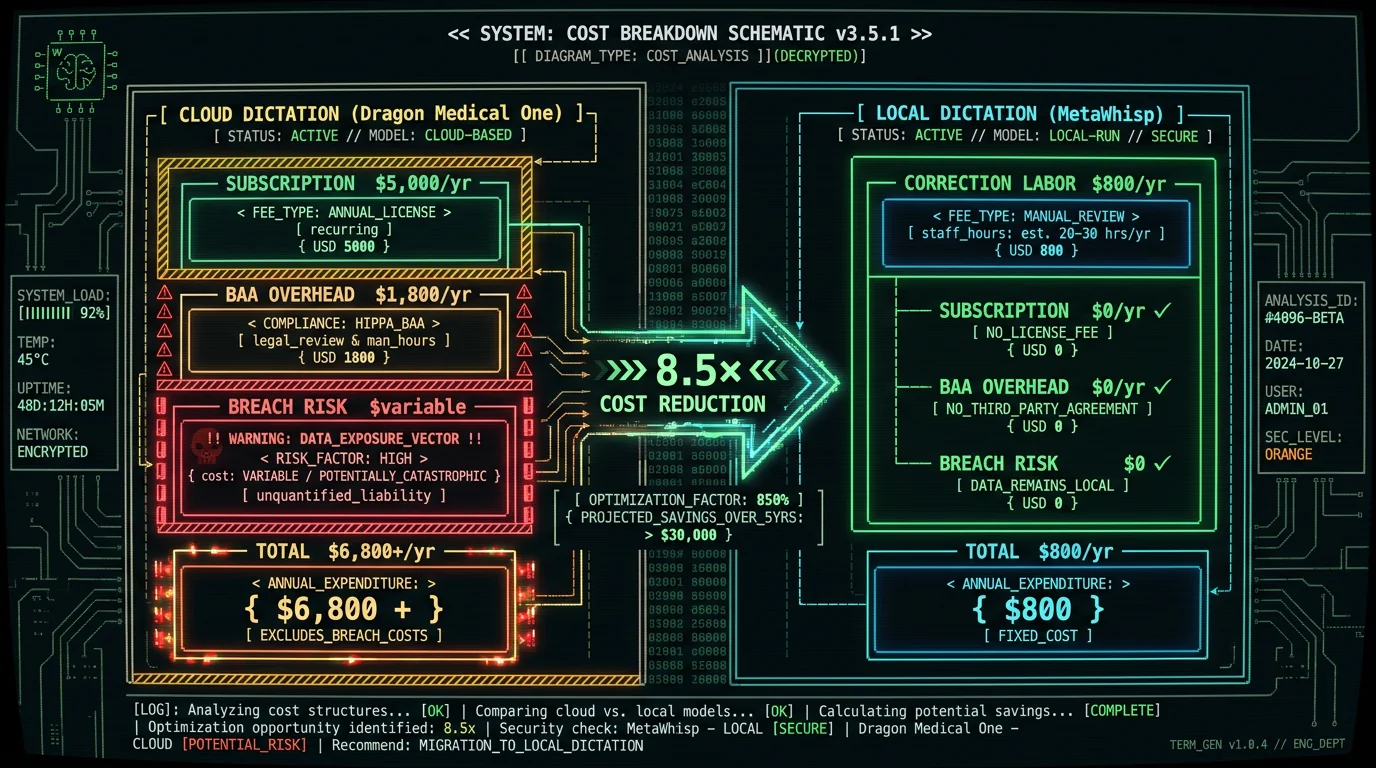
What Are the Hidden Costs of Cloud Dictation BAAs?
- Annual vendor security reviews: Your HIPAA Security Officer must assess each Business Associate's controls annually (§ 164.308(b)(1)). For Dragon Medical One, this includes reviewing Nuance's SOC 2 Type II report (40 pages), their subprocessor list (Microsoft Azure, 12 third-party services), and validating encryption standards. Budget 4-6 hours/year per vendor at $150/hour consulting rate = $600-900/year hidden labor cost.
- BAA amendment legal fees: Off-the-shelf BAAs often have unacceptable indemnification clauses, and negotiating an amendment (for example, to cap liability rather than accept an unlimited-liability template) typically means paying for legal review. Small practices skip this step and sign as-is, creating unquantified risk.
- Breach notification cascades: If Nuance suffers a breach, HIPAA requires you to notify affected patients within 60 days (§ 164.404). Notification costs (mail, call center, credit monitoring) average $240/patient per the IBM 2025 Cost of a Data Breach Report. A 5,000-patient breach = $1.2M in notification costs you pay, not the vendor.
- Audit response overhead: OCR HIPAA audits (random selection, ~200/year nationally) now include Business Associate chain audits. If your dictation vendor can't produce signed BAAs with their subcontractors (e.g., Azure ML API for model hosting), you get the deficiency notice. Remediation averages 40 hours of executive time + $15K in legal fees per the AMA's HIPAA Audit Preparation Guide (2024).
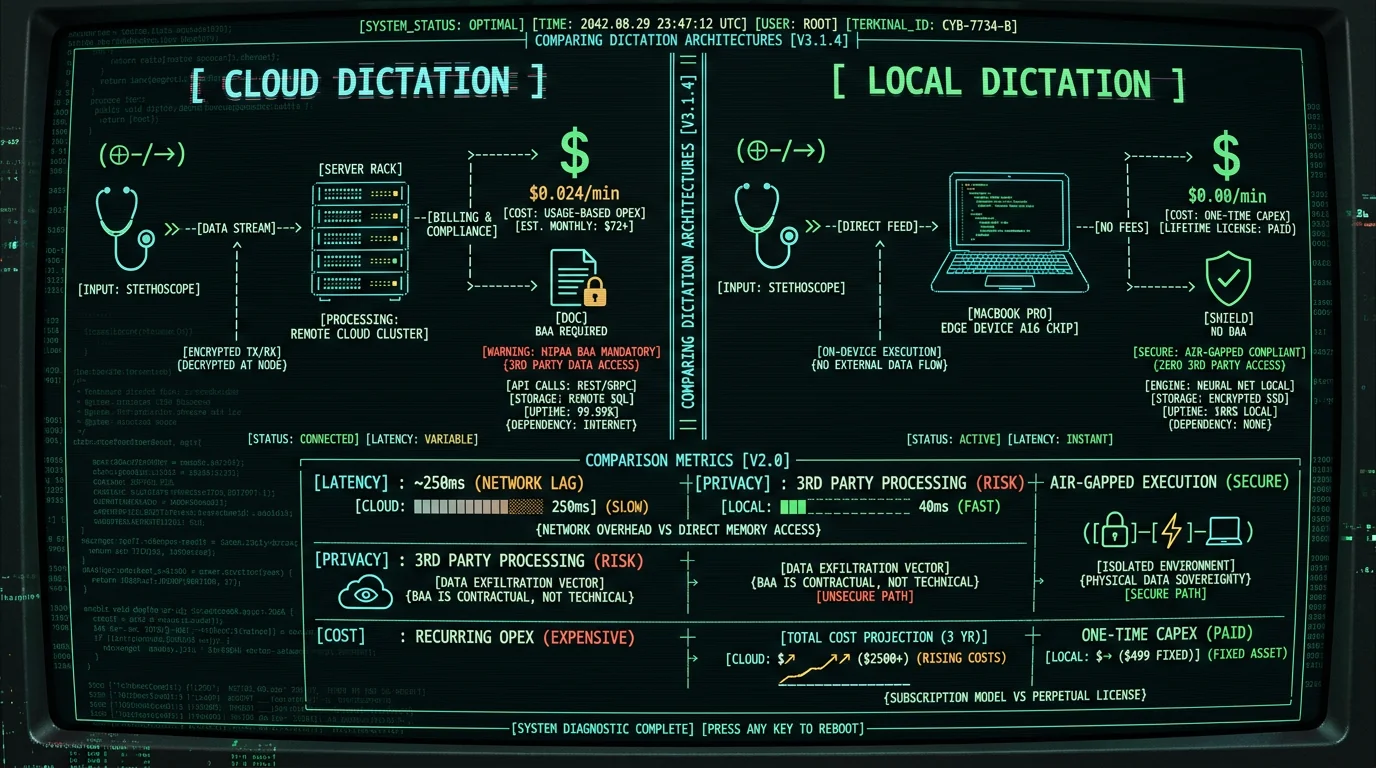
Cost contrast: a 10-provider practice on Dragon Medical One pays roughly $5K/year in subscription fees (at $500/provider), plus the ongoing BAA and vendor-review overhead. The same practice on MetaWhisp (free tier, offline mode) pays $0/year in licensing and has no BAA to maintain. A clinically-tuned tool like Dragon may need fewer manual corrections on dense terminology, which closes some of that gap. We haven't measured the trade-off on clinical audio, so the only honest way to compare is to test both on your own dictation.
How to Implement On-Device Dictation in Your HIPAA Workflow
Here's the deployment, step by step, for a solo practitioner or small practice:Download and install MetaWhisp in offline mode
Visit metawhisp.com/download, download the .dmg installer (small; the ~950 MB Whisper large-v3-turbo model downloads once on first launch). During first launch, System Settings → Privacy & Security → Microphone → enable MetaWhisp. In the app's settings, toggle Offline Mode to ON. This disables all network entitlements. Verify with Activity Monitor → Network: MetaWhisp shows 0 bytes sent/received.
Configure audit logging
Open Terminal, run log stream --predicate 'subsystem == "com.metawhisp"' --level debug > ~/Desktop/metawhisp_audit.log &. This captures all transcription events (start time, duration, word count, output file path, SHA-256 checksum) to a local log file. HIPAA § 164.312(b) requires audit trails for ePHI access. Rotate logs monthly, archive to encrypted external drive for 6-year retention (HIPAA minimum).
Test on non-PHI sample dictations
Dictate 10 fake patient notes (use fictional names, no real PHI). Verify transcripts appear in ~/Documents/MetaWhisp/, check accuracy against your most-used medications and procedures. Build a practice-specific custom vocabulary file (CSV format: "epinephrine,epi-NEF-rin" for phonetic hints). MetaWhisp reloads vocabulary files hot — no restart needed.
Document your HIPAA technical safeguards
Create a one-page Word doc titled "Dictation Software Technical Safeguards Assessment." Include: Tool name (MetaWhisp), processing architecture (on-device, no cloud transmission), BAA status (N/A — not a Business Associate), access controls (macOS user account permissions), audit controls (unified logging enabled), integrity controls (SHA-256 checksums on output). Sign, date, file in your HIPAA compliance binder. If OCR audits you, this documents how your setup helps address § 164.312.
Train your team on the 90-second rule
Unlike cloud tools, on-device processing has no session timeout. But medical assistants accustomed to Dragon's auto-punctuation may need retraining. MetaWhisp supports voice commands ("period", "new paragraph", "comma") but they must be spoken explicitly. Run a 15-minute training session: each clinician dictates one H&P, reviews output, adjusts speech pacing. Post a laminated "Dictation Best Practices" cheat sheet by each workstation.
What Happens If You Mix Cloud and Local Dictation Tools?
Can You Use On-Device Dictation for Telemedicine Notes?
Telemedicine muddies the picture, because the encounter happens over Zoom or Doxy.me and you're narrating the note during or right after the call. Dictate during the call and your voice is going to the telemedicine platform's cloud — a BAA event with Zoom. Dictate after the call (patient hangs up, you spend 3 minutes dictating the note into MetaWhisp) and it's on-device and HIPAA-compatible. The question that settles it: is the patient's audio being captured? If yes, you need the platform's BAA no matter which dictation tool you use. If no — you're talking to an empty room, patient off the line — on-device dictation keeps the PHI local. HHS's telehealth enforcement discretion (enacted March 2020, expired May 2023) is gone. As of 2026, any telemedicine platform that records or processes patient audio or video needs a signed BAA. That covers Zoom Healthcare, Doxy.me, Amwell — even FaceTime Audio if you use it for clinical encounters, since Apple's BAA only reaches enterprises with Apple Business Manager.Pro tip: Doing telemedicine? Dictate your note after the patient leaves the virtual room — on-device (MetaWhisp), while the call is still fresh. That keeps the BAA obligation on the telemedicine platform alone and off your dictation. And never dictate while the patient can still hear you. That's a privacy violation under § 164.530(c) (safeguarding PHI from incidental disclosures).
Which Medical Specialties Benefit Most from Local Dictation?
| Specialty | Primary Use Case | Cloud Risk | Local Dictation Fit |
|---|---|---|---|
| Psychiatry | Therapy session notes (30-60 min encounters) | High (sensitive mental health PHI, subpoena target) | ✅ Excellent (air-gapped, no 90-sec limit) |
| Surgery | Operative reports (5-15 min dictations, specialty terms) | Medium (PHI sensitivity, malpractice discovery risk) | ✅ Excellent (custom vocab for procedures) |
| Radiology | Imaging study reports (2-5 min, structured format) | Low (less narrative, more findings list) | ⚠️ Good (may prefer Dragon's templates) |
| Primary Care | Progress notes, H&P (10-15 min encounters) | Medium (high patient volume, breach notification exposure) | ✅ Excellent (fast turnaround, no per-note cost) |
| Legal Firms (depositions) | Attorney-client privileged transcripts (2+ hours) | High (attorney-client privilege = heightened confidentiality) | ✅ Excellent (see legal dictation guide) |
Frequently Asked Questions: HIPAA Local Dictation on Mac
Is on-device Whisper as accurate as Dragon Medical One?
Dragon Medical One is built for clinical vocabulary and ranks among the most accurate medical dictation tools out there. It's also paid, cloud-based, and needs a BAA. MetaWhisp runs general-purpose Whisper large-v3-turbo entirely on-device, for free. We haven't run a controlled head-to-head on clinical audio, so we won't quote an accuracy gap. The honest version: a specialized paid tool like Dragon may handle dense jargon better out of the box, while MetaWhisp gives you on-device privacy at zero cost. High-acuity specialties — trauma surgery, oncology — where a transcription error carries malpractice risk may still prefer Dragon's domain tuning despite the compliance burden and the price.
Do I need a BAA with Apple for using MetaWhisp on macOS?
No. MetaWhisp is a third-party app that runs on macOS but doesn't send PHI to Apple. You don't need an Apple BAA unless you're syncing transcripts through iCloud Drive (don't) or using Apple's Server-Based Dictation (avoid it for HIPAA). Keep MetaWhisp transcripts on the Mac's internal SSD and no Apple BAA applies. The one case where you'd need a BAA: backing the Mac up to a cloud service like Backblaze or Dropbox. Then the BAA is with that vendor.
Can I dictate prescriptions into MetaWhisp and have them auto-populate my EHR?
Not directly. MetaWhisp outputs plain text. Integration with EHRs (Epic, Cerner, Athenahealth) needs HL7 FHIR API calls, which MetaWhisp deliberately doesn't implement — that's how it stays off the cloud. What you can do: copy-paste transcripts into your EHR's note field, or use macOS Shortcuts to auto-fill structured data. Real EHR integration means middleware — say, a Python script that parses MetaWhisp's output and POSTs to your EHR's API. And that middleware has to be HIPAA-audited too.
What happens if my Mac is stolen? Is PHI encrypted at rest?
macOS FileVault (System Settings → Privacy & Security → FileVault) encrypts your whole disk with XTS-AES-128. Turn it on and MetaWhisp transcripts in ~/Documents/ are encrypted at rest. If the Mac gets stolen with FileVault on, the thief can't reach any PHI without your login password. HIPAA § 164.312(a)(2)(iv) addresses encryption or an equivalent alternative measure, and FileVault helps address it. Enable it before you store any PHI. One catch: if you run Time Machine backups to an external drive, that drive has to be encrypted too (Disk Utility → Erase → APFS Encrypted).
Can I use MetaWhisp on an M1 MacBook Air or do I need an M3 Max?
The M1 MacBook Air (2020, 8-core CPU, 7/8-core GPU, 16-core Neural Engine) runs Whisper large-v3-turbo faster than real time — fine for typical clinical notes. M3 Pro/Max chips are faster still, which trims the wait on long dictations like 30-60 minute psychiatric intakes or 2-hour surgical op reports. RAM matters more than the exact chip, though. 16 GB unified memory is the sweet spot; 8 GB Macs may swap to disk mid-transcription and slow down noticeably.
Does MetaWhisp support real-time transcription (live text appearing as I speak)?
Yes. Turn on streaming mode in settings. Whisper works in 30-second audio chunks, so text lands in ~2-second bursts rather than word-by-word like Dragon. Speech-to-text latency runs 40-60 milliseconds on M3 chips. If you need instant visual feedback — dictating while reviewing a radiology image, say — streaming mode is the one you want. If you dictate the whole note and review it after (post-call documentation), batch mode is faster.
Can I share my fine-tuned Whisper model with my partner physicians without violating HIPAA?
Yes — if the fine-tuning audio contained no PHI, or if PHI was de-identified per § 164.514(b) (remove 18 identifiers). The model file itself, the weights and parameters, holds no PHI. It's a statistical artifact. But if you fine-tuned on real patient dictations with names and dates, and someone could in theory reconstruct those names from the model (the emerging "model inversion" attacks), you're in a gray area. Safest path: fine-tune on synthetic data — fake patient names generated by GPT-4, real medical vocabulary. Then the model is unambiguously shareable.
What if I need to dictate in Spanish for my bilingual patient population?
Whisper large-v3-turbo supports 99 languages, Spanish among them. In MetaWhisp settings, pick "Spanish (es)" as the input language. The model auto-detects language per 30-second chunk, so you can code-switch mid-sentence ("The patient presented with dolor abdominal and náuseas") and Whisper rides the shift. Medical Spanish — drug names, anatomy terms — is harder than everyday speech, and we haven't run a controlled clinical-Spanish benchmark, so test it on your own dictation. For practices with a heavy non-English caseload, bilingual dictation on-device sidesteps the cloud services that bill per language.
Is MetaWhisp certified for Meaningful Use / Promoting Interoperability?
Meaningful Use (now "Promoting Interoperability") certification applies to EHR systems, not dictation tools. MetaWhisp isn't an EHR and doesn't need ONC-ACB certification. But if your EHR's PI requirements call for "≥90% of clinical notes created via CPOE or voice recognition," MetaWhisp transcripts you copy-paste into Epic or Cerner satisfy the "voice recognition" criterion. Keep your MetaWhisp audit logs as evidence of note creation method for PI attestation.
Can I use MetaWhisp for research transcription (interviews with human subjects)?
Yes. IRB-approved research with audio recordings of human subjects carries HIPAA-like requirements (45 CFR 46, the Common Rule). If your IRB protocol says "audio data will not leave the institution," on-device transcription meets it. Plenty of universities ban cloud transcription services like Rev.com and Otter.ai for IRB studies, purely because of BAA complexity. MetaWhisp's offline mode fits IRB rules: no data transmission, local storage, auditable. Check your IRB's data security plan template — "on-device Whisper" is a perfectly good answer to "How will audio be transcribed?"
Author's Take: Why I Built MetaWhisp for HIPAA Workflows
I'm Andrew Dyuzhov, solo founder of MetaWhisp. I built this because the math on cloud medical dictation never added up for me. You pay a recurring per-seat fee and babysit BAA paperwork for a service that, on modern Apple Silicon, can run entirely on your own machine. When OpenAI released Whisper in December 2022, on-device transcription stopped being a research demo and became something you could actually use day to day. The regulatory logic is simple: if PHI never leaves the device, an entire transmission-based compliance category just disappears. Getting Whisper to run well on Apple Silicon took real engineering — Core ML conversion, quantization, Neural Engine dispatch — and the result runs comfortably faster than real time, costs $0, and needs no BAA paperwork.
This isn't anti-cloud ideology. It's pragmatism. Cloud dictation made sense back when local CPUs couldn't run real-time ASR. They can now — Apple's Neural Engine handles Whisper inference on-device fast enough for live dictation. So local is competitive on speed, cheaper, and simpler on compliance. The two real reasons to stay on cloud are domain-tuned accuracy for dense clinical vocabulary and existing workflow lock-in. Both legitimate. Both worth weighing against the cost and the compliance overhead.
If you're a clinician thinking "I don't have time to evaluate new tools" — I get it. But 30 minutes with MetaWhisp could retire a recurring per-seat subscription and the BAA overhead that rides along with cloud dictation. Download the free tier, dictate a handful of patient notes in offline mode, and compare the output to Dragon on your own vocabulary. If it's accurate enough for your specialty, you've found a HIPAA-compatible off-ramp from the subscription treadmill. If it isn't, you're out 30 minutes and nothing else.
Related Reading
- Medical Dictation for Doctors: HIPAA Compliance in 2026 — Deep dive on PHI protection, BAA requirements, and audit logging for clinical documentation workflows
- Voice-to-Text for Lawyers on Mac: Attorney-Client Privilege Protection — How legal professionals use on-device Whisper to keep depositions and case notes confidential
- On-Device Transcription: How MetaWhisp Runs Whisper Locally — Technical breakdown of Core ML optimization, Neural Engine dispatch, and real-time performance benchmarks
- MetaWhisp Processing Modes: Streaming vs. Batch Transcription — When to use real-time mode (psychiatric intakes, surgical dictation) vs. batch mode (post-call documentation)